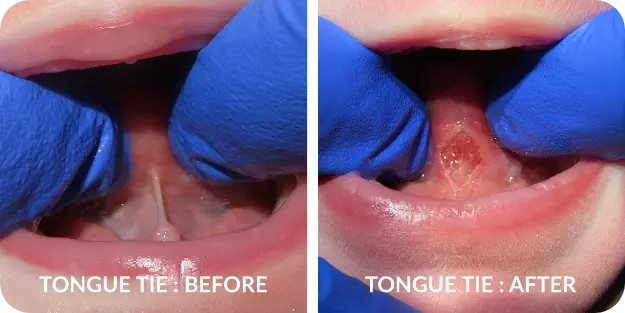
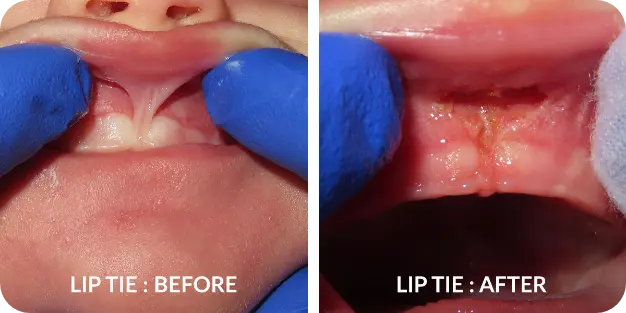

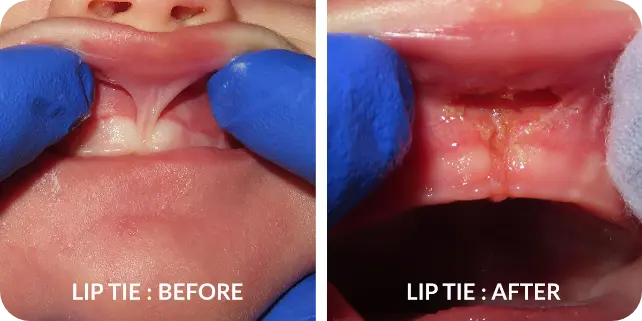
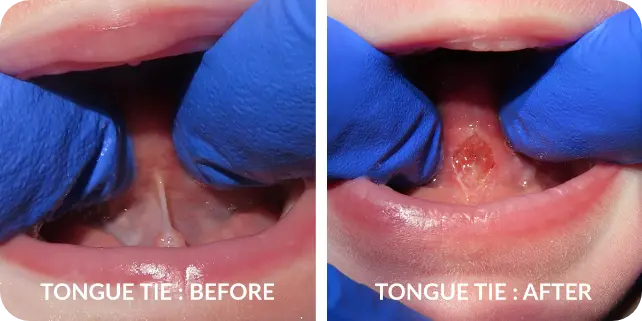
The medical term for tongue tie is ankyloglossia. It’s a fancy word that describes a simple concept. Picture your baby with his or her mouth wide open, tongue curled back so you can see the bottom of the tongue. There’s a “cord” running down the center of the bottom of the tongue. That’s a ligament that attaches the tongue to the bottom of the mouth. It’s called a lingual frenum or frenulum. When the frenulum is too short and/or too thick, it “ties” the tongue to the floor of the mouth. This restricts tongue motion, impairs tongue mobility and can cause a host of functional and developmental problems for the tongue tied baby. A simple analogy is a baby being born with webbed fingers or toes– this child will have to learn to use their body differently to make up for the lack of normal function and may have lifelong repercussions.



Infants typically do not require any type of sedation for a frenectomy. Your baby will be swaddled, protective eyewear placed, and either one or two assistants will keep your baby safe and still. Keep in mind that the laser is very precise and controlled, and is very safe even on a crying infant.
For older babies and children, each situation is evaluated on a case by case depending on symptoms, urgency, physical and emotional well being of your child. For older children we may use a combination of laughing gas, a movie, and numbing.
The short answer is yes! During your appointment we will thoroughly discuss, demonstrate, and give written instructions on home care as we have found it is critical for the success of the frenectomy.